If you think modern medicine has its share of horror stories, wait until you hear about the surgeon who somehow managed to kill three people during a single operation — and the patient wasn’t even one of the first to go. It sounds like a dark comedy sketch, but it’s a true chapter from the history of surgery, one that reveals just how terrifying, chaotic, and primitive the operating theater once was. The name at the center of this grim record is Robert Liston, and his legacy is one of the strangest contradictions in all of medical history: a man celebrated as the fastest, most skilled surgeon of his era who also holds the dubious distinction of having achieved a 300% mortality rate in a single procedure.
Before you dismiss that figure as an exaggeration, consider this — three people died as a direct result of one operation. The patient, the assistant, and a bystander. One surgery. Three deaths. Do the math, and you get something that should be statistically impossible: a mortality rate that exceeds 100%. Yet here we are, writing about it centuries later, still shaking our heads.
Who Was Robert Liston? The Man Behind the Blade
Robert Liston was born in 1794 in Ecclesmachan, a small village in Scotland, and from an early age he demonstrated an almost supernatural aptitude for the medical arts. He studied surgery in Edinburgh under some of the finest anatomists in Britain, and it quickly became clear that this young man had hands built for the operating table. His physical presence alone was remarkable — tall, powerfully built, with enormous hands and fingers that could grip bone and flesh with an almost mechanical certainty. Surgeons in the early nineteenth century needed physical strength as much as technical skill, and Liston had both in abundance.
He eventually moved to London, where he took up a position at University College Hospital, and it was there that his reputation truly exploded. Colleagues admired him. Patients feared him, but lined up anyway. Medical students idolized him. At a time when surgery was only beginning to shed its reputation as a last-ditch act of desperation, Liston was turning it into something approaching a spectacle of human capability. He was precise, he was confident, and above all, he was breathtakingly fast.
Speed, in the pre-anesthetic era, was not a vanity — it was a mercy. Patients were conscious during operations, held down by assistants, screaming through every cut. The faster a surgeon worked, the less suffering a patient endured. A slow surgeon was a cruel surgeon, at least by the standards of the time. Liston understood this deeply, and he made speed the centerpiece of his craft. He didn’t just operate quickly for the sake of showmanship; he operated quickly because he genuinely believed that reducing the duration of agony was a moral obligation.
His technique was studied and refined over years of practice, and by the time he was at the height of his career, he could amputate a leg at the thigh in under thirty seconds. Not thirty minutes — thirty seconds. Contemporary accounts describe audiences in the gallery of the operating theater genuinely struggling to follow his movements with their eyes. He moved with a fluidity that seemed impossible for the brutality of the task at hand.
Surgery Before Anesthesia: A World of Screaming and Speed
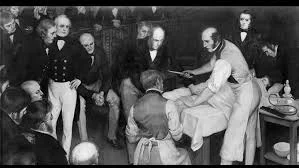
To truly appreciate Robert Liston’s context — and the catastrophe that would come to define his legacy — you need to understand what surgery looked like before the mid-nineteenth century. There was no general anesthesia. There were no sterile gloves, no antiseptics in regular use, no understanding of germ theory. The operating theater was exactly that: a theater, complete with gallery seating for students, observers, and even members of the public with a strong enough stomach.
Surgeons wore their blood-stained coats as badges of honor. A coat thick with old, dried blood was proof of experience, proof of volume, proof of a career spent in the trenches of human suffering. The notion of washing hands between patients would have seemed absurd to most practitioners of the era — not because they were careless, but because the connection between microbial contamination and infection simply hadn’t been established yet. That understanding would come later, largely through the work of figures like Joseph Lister and Ignaz Semmelweis, but in Liston’s operating room, the germ was still an unknown enemy.
Patients who faced surgery dreaded it with a visceral terror that is almost incomprehensible by modern standards. Accounts from the period describe men and women weeping, praying, and making final arrangements before going under the knife — and with good reason. Even if a surgeon was technically successful, post-operative infection killed a staggering proportion of patients. The operating table was genuinely a place where you might go to die, and many did. Under these conditions, the surgeon’s speed wasn’t just a technical preference — it was one of the only real tools he had to tip the odds in a patient’s favor.
Liston thrived in this environment. He cut through tissue with an economy of motion that his contemporaries could only marvel at. He had developed a grip so firm and so practiced that his blade seemed to find its own path. Colleagues described watching him operate as something close to watching a master craftsman at work — horrifying in its subject matter, but undeniably beautiful in its execution. The operating theater at University College Hospital was packed whenever Liston was scheduled to operate, and the energy in the room was closer to a sporting event than a medical procedure.

The Infamous Operation: How One Surgery Killed Three People
And now we arrive at the story that history simply cannot let go of. The precise date of the operation varies depending on the source, but it took place in the 1840s in London, during an amputation of a patient’s leg. Liston was at the peak of his powers, and the gallery was filled with observers eager to watch the master at work. Everything about the setup was normal. The patient was prepared, the instruments were laid out, and Liston took his place at the table.
What followed happened so fast that witnesses could barely piece together the sequence of events in the immediate aftermath. Liston began the amputation with his characteristic blinding speed, drawing the blade through flesh and bone in a series of confident, sweeping motions. He was moving so quickly, so completely locked into the rhythm of the procedure, that his attention was focused entirely on the surgical field in front of him.
In the process, the blade moved faster than the assistant’s hands could follow. Liston’s knife sliced through his patient’s leg — and in the same motion, accidentally amputated several fingers of the assistant who was helping to hold the limb in place. The assistant, shocked and suddenly bleeding heavily, had no time to react before the damage was done. Liston, still moving at full speed, may not have even fully registered what had happened until the cut was complete.
Somewhere in the gallery, among the assembled students and observers, a man watching the procedure was standing close enough to see the flash of the blade and feel the spray of blood. He apparently believed, in the chaos of that moment, that he too had been cut — that Liston’s knife had somehow reached into the gallery and found him. The psychological shock was so severe that he collapsed on the spot and died of what was determined to be a heart attack.
Then the slow tragedy began to unfold. In the days that followed, both the patient and the assistant developed infections — blood poisoning, as it was commonly described at the time, which was the era’s general term for what we would now recognize as sepsis. Despite whatever efforts were made to treat them, both men died. The patient whose leg had been amputated. The assistant whose fingers had been taken. Two deaths from a single operation, on top of the spectator who had already died from fright.
Three people. One operation. A mortality rate of 300%.
Why Speed Became Liston’s Downfall in That Moment
There is a painful irony at the heart of this story. The very quality that made Robert Liston exceptional — his extraordinary speed — was the direct cause of the catastrophe. Speed, in the pre-anesthetic age, was perhaps the single most valuable attribute a surgeon could possess. Liston had cultivated it over decades of practice, honed it to a degree that no one else in his generation could match, and used it to spare countless patients unnecessary suffering. And yet, in that one operation, the same speed that had saved lives became the mechanism of disaster.
What the incident reveals is something that modern surgical training has absorbed as a foundational lesson: technical skill, no matter how extraordinary, must be paired with situational awareness. A surgeon who moves faster than their team can safely follow is a surgeon who has lost the plot, however briefly. The assistant’s fingers were in the wrong place, or perhaps in the right place and simply unable to move in time. The result was the same either way.
It’s also worth noting that Liston himself was not a reckless man by the standards of his era. He was not performing that operation carelessly or showing off for the gallery, despite what the dramatic retelling might suggest. He was doing exactly what he always did — moving with maximum efficiency to minimize his patient’s suffering. The tragedy was systemic as much as it was personal. In a world without anesthesia, the pressure to operate fast created a dangerous incentive structure, one where the margin for error was compressed to almost nothing.
After this incident, Robert Liston’s career continued — he was too skilled and too respected for one catastrophic operation to end his professional life. He also lived to see the introduction of ether anesthesia, which transformed surgery almost overnight and removed the brutal calculus of speed that had defined his entire approach to medicine. He reportedly embraced it with genuine enthusiasm, understanding immediately what it meant for his patients. He died in 1847, just a year after ether was first used in Britain, and the age of the speed surgeon died with him.
The Operating Theater as a Stage: Medicine and Spectacle
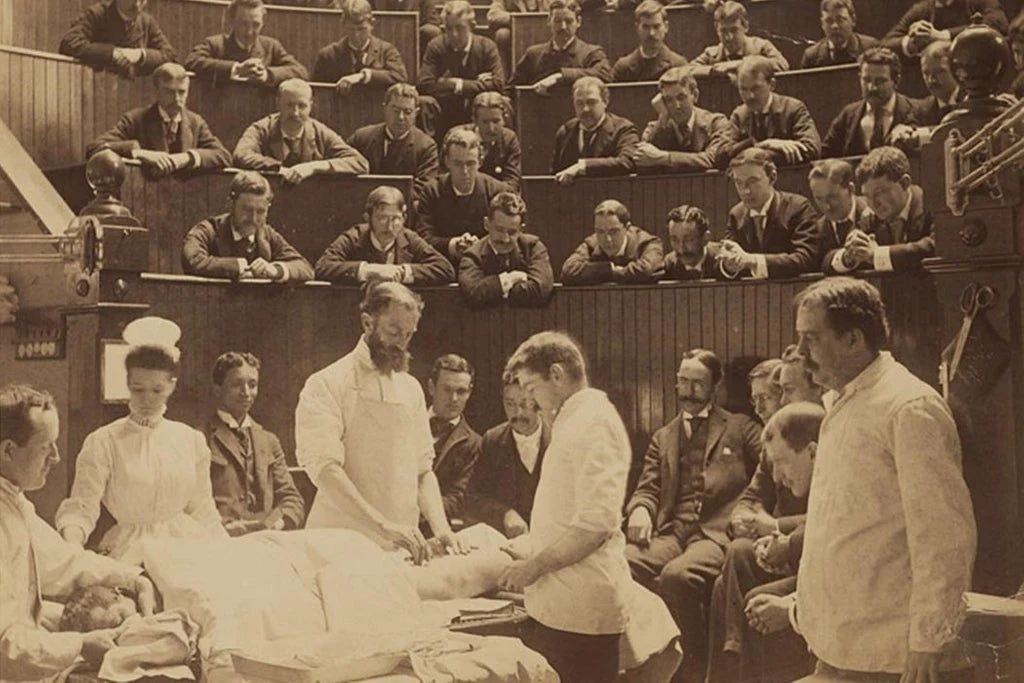
One dimension of this story that often gets overlooked in favor of the grim arithmetic is the theatrical dimension of early nineteenth-century surgery. The operating theater was, quite literally, a place of performance. Tiered seating allowed dozens of spectators to watch procedures from above, and the surgeon occupied a stage-like floor where his every movement was visible to the assembled crowd. Medical students came to observe and learn. Curious members of the public sometimes attended. The atmosphere was charged, intense, and in its own way, deeply strange.
Liston was a performer in this environment whether he intended to be or not. His reputation preceded him into every operating theater he entered, and observers came specifically to watch him work. The sheer theatrical impact of seeing a limb removed in under thirty seconds, with a confidence and precision that seemed almost inhuman, left witnesses with accounts that were passed down through generations of medical students. He was not merely a surgeon; he was an event.
This theatrical context helps explain why the presence of a non-medical bystander in the gallery on the day of the infamous operation was entirely normal. The gallery was a public space of sorts, and the operating theater functioned as an educational and social institution simultaneously. The fact that a spectator died of a heart attack during the procedure, while tragic, was not entirely unprecedented in the sense that the gallery attracted all types — some with the constitution for what they were about to see, and some without.
What the story also illustrates is the degree to which medicine, in this period, had not yet fully defined the boundaries between clinical practice and public performance. The pressures that created a surgeon like Liston — who moved at terrifying speed in front of a paying audience — were in part social and theatrical pressures, not purely clinical ones. The transition to closed operating rooms, scrubbed sterile environments, and procedures performed in the absence of gallery audiences was a transformation not just of technique but of philosophy.
Robert Liston’s Real Legacy: A Pioneer at the Turning Point
Despite the morbid curiosity that tends to dominate retellings of his story, Robert Liston was genuinely one of the most important surgical figures of the nineteenth century, and his contributions to medicine deserve to be recognized alongside the dark comedy of his worst day. His speed and technical precision saved countless lives during a period when the alternative to a fast amputation was frequently a slow, agonizing death. He operated at a time when the mortality rate for major surgery was terrifyingly high, and his outcomes were, by the standards of his era, actually quite good.
Liston was also one of the first surgeons in Britain to use ether anesthesia, and his willingness to embrace a paradigm-shifting new technology speaks well of his intellectual flexibility. When ether was demonstrated at University College Hospital in December 1846, it was Liston who performed the first operation under its influence in Britain, amputating a leg with the patient fully unconscious. He reportedly turned to the assembled observers afterward and said words to the effect of: “This Yankee dodge beats mesmerism hollow.” It was a typically terse and confident pronouncement, and it marked the end of one era of surgery and the beginning of another.
His surgical textbook, “Practical Surgery,” published in 1837, was widely read and influential, laying out principles and techniques that shaped the training of a generation of surgeons. He was a gifted teacher as well as a practitioner, and many of his students went on to distinguished careers of their own. The professional network he helped build at University College Hospital became one of the anchors of British medical education in the Victorian era.
To reduce Robert Liston to the surgeon who achieved a 300% mortality rate is, in a sense, to make the same mistake that all good historical storytelling risks — taking the most sensational moment in a life and letting it stand in for the whole. His whole career was far more complex, far more impressive, and in its way far more humanly interesting than any single operation, however catastrophic, can capture.
What This Story Teaches Us About the History of Medicine
The Robert Liston story has endured in medical folklore for nearly two centuries because it captures something essential about the nature of progress. Medicine does not advance in a straight line from ignorance to enlightenment. It lurches forward through catastrophe and accident, through brilliant individuals operating in conditions of profound uncertainty, and through the slow accumulation of failures that eventually make success more likely. The 300% mortality rate is a grotesque artifact of an era when surgeons had almost none of the tools we now take for granted, and when the best thing a healer could offer was speed.
The story also serves as a reminder that the metrics we use to evaluate success and failure are always embedded in the assumptions of their time. Speed was a rational optimization in Liston’s world. The fastest surgeon was, by the logic of his era, the most merciful surgeon. That logic was not wrong — it was simply incomplete. The introduction of anesthesia didn’t reveal that Liston had been doing it wrong; it revealed that the entire framework within which he had been operating was obsolete. He was the best possible version of something that the world was about to stop needing.
Modern surgical training has absorbed these lessons in ways both explicit and implicit. The sterile field, the scrubbed team, the anesthesiologist, the instrument count, the strict protocols around counting sponges and blades — all of these are responses, however indirect, to the cascading disasters that could unfold when a surgeon moved faster than his environment could safely support. The choreography of a modern operating room is designed precisely to prevent the kind of momentum-driven catastrophe that claimed the fingers of Liston’s assistant.
Yet there is something almost noble in the image of Liston at the table — a big, fierce, supremely skilled man doing the most terrifying thing imaginable with absolute commitment, trying his best to be the fastest mercy his patients had ever known. He was a creature of his time, doing what his time demanded of him. That he occasionally did it too well is part of what makes him unforgettable.
Conclusion: The Fastest Blade and Its Terrible Price
Robert Liston remains one of the most fascinating figures in the history of surgery — celebrated, notorious, and impossible to forget. He was a genuine pioneer, a master of his craft who practiced at one of the most demanding crossroads in the history of medicine, when the tools of healing were primitive and the stakes were absolute. His extraordinary speed saved patients from prolonged agony at a time when prolonged agony was frequently a death sentence. And in one catastrophic operation, that same speed created a chain of events so improbable that it has been retold in every generation since.
The 300% mortality rate is not just a macabre piece of trivia — it is a window into a world where surgery was simultaneously life-saving and life-threatening, where the operating theater was as much a stage as a clinic, and where the best intentions and the worst outcomes could inhabit the same thirty-second blur of blade and bone. Robert Liston deserves to be remembered not as a failure, but as a symbol of medicine at its most heroic and most human — brilliant, flawed, moving as fast as it possibly could, and not quite fast enough to outrun its own limitations.
Historical Period Classification: The events described in this article belong to the Early Modern period of history, specifically the first half of the nineteenth century (approximately 1820s–1847). This era bridges the tail end of the Enlightenment and the beginning of the modern scientific revolution in medicine, predating the germ theory of disease, the widespread adoption of antiseptic technique, and general anesthesia — all of which would transform surgery into something recognizably modern within a generation of Liston’s death.